Extremity Trauma
Limb injuries following trauma are extremely common ED presentations.
Some limb injuries can be life threatening
- External exsanguination from arterial bleeding
- “internal bleeding” from femoral or other long bone fractures
- an adult can bleed 1.5L from a single femoral #
- crush syndrome
Other limb injuries are “limb” threatening
- mangled limbs and amputations
- neurovascular injuries
- compound fractures
- compartment syndrome from crush injures, fractures, burns
- degloving injuries
Note that in polytrauma patients, a seemingly “minor” missed injury (eg: base of thumb fracture) can lead to significant long term disability.
Hence a thorough secondary and tertiary survey is essential after life and limb threats have been identified and treated.
Principles of management
1. Address immediate life-threatening injuries
External exsanguination
Exsanguinating haemorrhage from extremity trauma should be managed as a priority during the primary survey.
Many trauma providers advocate a “CABC” approach with the first “C” being – control external exsanguination.
If extremity bleeding cannot be stopped with firm direct pressure, a tourniquet should be applied. The most commonly utilised tourniquet in the Northern Region is the “CAT” (combat application tourniquet)
Click on this link for a video on CAT application https://www.narescue.com/combat-application-tourniquet-c-a-t-instructions.html

The Combat Application Tourniquet (CAT)
Principles of tourniquet application
– cut off clothes from the affected limb
– apply a few centimetres proximal to the wound
– don’t apply over a joint
– tighten until bleeding is controlled
– note the time of application
– if still bleeding – place a 2nd tourniquet proximally
- A tourniquet should only be left on for 2 hours before it needs to be released to allow perfusion of the distal limb.
- Be prepared to apply direct pressure to the bleeding area after release of the tourniquet.
- Provided that direct pressure can adequately control any bleeding, the tourniquet should be kept off for 20 minutes.
- The tourniquet can be reapplied if bleeding is an ongoing concern.
AT MIDDLEMORE HOSPITAL – if a tourniquet is required for haemorrhage control a RED BLANKET should be initiated in consultation with the on-call Vascular and/or Plastic/Hands (forearm, wrist or hand) Surgeon.
If the bleeding can be controlled with direct pressure a device known as “The Emergency Bandage” (aka The Israeli Bandage) can be utilised. It is a compression bandage with a built in pressure bar. Some departments may stock this. St John have an education sheet which you can read more about this dressing – click on this link for more information.

The Emergency (Israeli) Bandage
Long bone fractures
Early reduction of long bone fractures will decrease bleeding by bringing the bony ends together. In terms of volume of blood loss, this is most important for femoral fractures. Various traction devices are available. Reduction of fractures is extremely painful – give adequate analgesia/sedation and consider utilising regional nerve blocks (eg: femoral nerve block)
Treat crush syndrome
Crush syndrome occurs when a body part is released after a period of entrapment. In general, one limb needs to be crushed for 1 hour for this to occur.
Release causes the circulation to be flooded with lactate, potassium and vasoactive oxygen free radicals from the injured cells and can trigger lethal cardiac dysrhythmias and hypovolaemic shock. Release of myoglobin can cause acute kidney injury.
Treating crush syndrome will usually be a pre-hospital consideration (immediately after the affected area is released) but patients may arrive to ED following extrication with limb tourniquet in situ (placed pre-hospital to limit the effects of crush syndrome from a release limb) or have ongoing sequelae from release.
Initial management of crush syndrome
- IV fluids to maintain urine output 2-3ml/kg/h
- Treat hyperkalaemia
- 10ml 10% calcium gluconate boluses over 2-5 minutes
- 10U actrapid insulin + 50ml 50% dextrose
- Salbutamol nebulisers 5mg
- Sodium bicarbonate 1 mmol/kg
2. Address limb threatening injuries
Mangled limbs and amputation
Mangled limbs can be defined as “any extremity sustaining sufficiently severe injury to a combination of vascular, bony, soft tissue and/or nerve structure that results in subsequent concern for viability of the limb”1
Mangled limbs need to be assessed for viability and urgently referred to an appropriate facility after other life threats have been addressed. All upper limb mangled extremities that not in extremis (dying) need urgent discussion with the Hands/Plastics service at Middlemore hospital for consideration of salvage/replant. Severely mangled feet and distal tibiae can be assessed and potentially primarily amputated by the nearest Orthopaedic service in the first instance. They should have a low threshold for discussion with the on call Orthopaedic and Plastic surgical consultants at Middlemore Hospital for consideration of salvage. All other proximal lower leg injuries require referral to the appropriate service/destination (see below)
Amputations can be partial or complete. Some upper limb complete amputations can be replanted – in general there is a 6 hour “cold ischaemia” window to reattach (though may be longer in some circumstances). Incomplete amputations are more time sensitive than complete amputations.
Management of complete amputations of the upper limb
Handle the amputated part with care – do not debride. Irrigate with normal saline and wrap loosely in saline soaked gauze. Place in a water tight bag then put bag into an ice slurry. Ice should never contact the amputated part directly. Label the part and the bag.
The stump portion should have bleeding controlled (may require a tourniquet), be irrigated and covered in saline soaked gauze. Treat with patient with antibiotics (as per “compound fractures” – see below) and update tetanus as required.
After life threats have been identified and managed, refer as soon as possible to the appropriate surgical service (Hands/Plastics service)
Neurovascular injury
Following trauma, all limbs should have their neurovascular status assessed after reduction of fracture, warming and resuscitation.
This involves checking
- Pulses
- If not immediately palpable, check using doppler
- Note that a palpable pulse does not exclude arterial injury. Certain injury patterns (eg: knee dislocation – popliteal artery injury) should spark a high index of suspicion and further tests (eg: CTA run off) should be considered
- Capillary return
- Sensation
- Motor power as best able
The clinician should be aware of injury patterns that are associated with various limb injuries eg:
- Knee dislocation: popliteal artery injury, peroneal and tibial nerve injury (beware that the dysaesthesia of nerve injury can mask the pain of compartment syndrome and/or ischaemia).
- Mid-shaft humerus fracture: radial nerve injury
Open (Compound) fractures
Compound (aka: open) fractures place the patient at risk of infection, repeat operation, eventual amputation and chronic disability due to communication of the fracture site with the outside world.
Management
- Control haemorrhage
- Reduce, remove gross debris , photograph and splint (with adequate analgesia/sedation)
- Assess and document neurovascular status
- Cover wound with moist dressing – please photograph first to avoid repeated exposure/ inoculation
- Antimicrobial cover as per local guidelines
Middlremore Open Fracture Antibiotic Guideline
This table outlines empiric antibiotic coverage for immediate management of open fractures
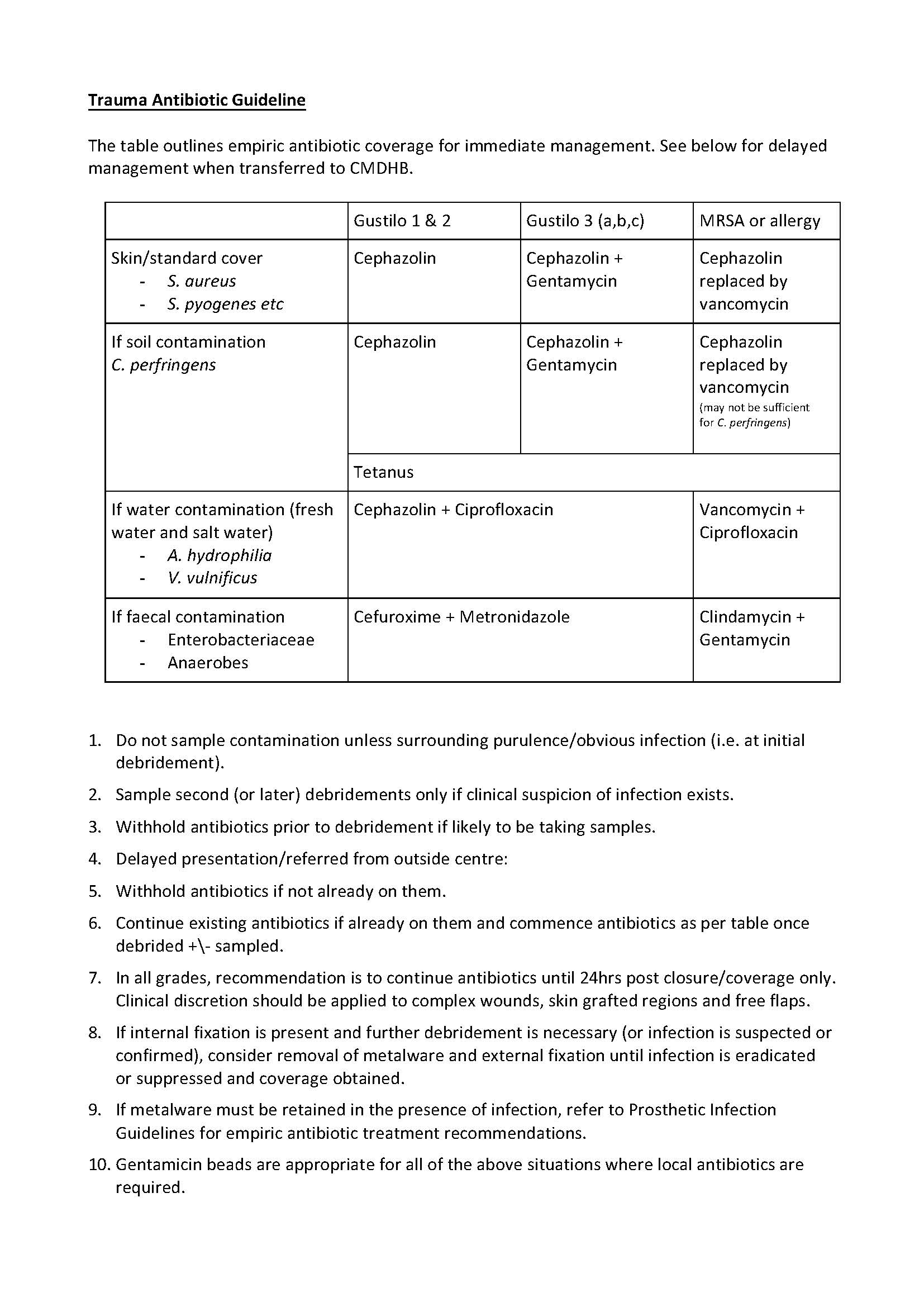
Click HERE for more information on the Gustilo classification
Notes:
- Give antibiotics as early as possible after injury, but delay Gentamicin until fluid resuscitated.
- Do not sample contaminants/debris at initial debridement unless there is surrounding purulence/obvious infection. Biopsy only when there is suspicion of infection.
- In all grades, recommendation is to continue antibiotics until 72hrs post closure/coverage only. Clinical discretion should be applied to complex wounds, skin grafted regions and free flaps.
- Gentamicin beads are appropriate for all of the above situations where local antibiotics are required.
- Give tetanus toxin or immunoglobulin as indicated (open fractures are tetanus prone wounds
- For grade 1 and 2 fractures, arrange operative washout and debridement with on call Orthopaedic service.
- Recent meta analysis clearly shows that in high grade open lower limb fractures, a longer time to debridement results in worse outcomes. This must be balanced against the risks of emergent surgery in the under-resuscitated or under-investigated patient.
- For grade 3 fractures, see Soft tissue defects in lower limb fractures below
Compartment syndrome
High pressures within a limb muscular compartment bound by fascia can lead to decreased tissue perfusion with subsequent irreversible nerve injury and muscle necrosis. Rhabdomyolysis and acute kidney injury can also occur as a result. Long term complications include ischaemic contractures and disability.
In terms of crush injuries, the risk of traumatic rhabdomyolysis leading to myoglobinuria and acute kidney injury (and even sudden cardiac death) is directly proportional to the number of limbs crushed. Central crushes have a high mortality. The treatment of myoglobinuria is fluids aiming for a urine output of 2-3ml/kg/hr. Haemodialysis may be required if the patient develops a severe AKI with persistent metabolic disturbance.
The presence of an open fracture does not exclude compartment syndrome occurring.
Causes of compartment syndrome include
- Fractures (especially lower limb and forearm)
- Crush injuries
- Penetrating trauma
- Acute blunt trauma with severe haematoma causing impaired arterial inflow locally
- Prolonged immobility with altered level of consciousness (e.g. drug induced)
- Burns (high voltage electrical)
- Minor injuries in patients with bleeding diatheses or on anticoagulants
Symptoms and signs of compartment syndrome (the “P”s)
- Pain out of proportion to the apparent injury
- this is the most sensitive sign, but beware of the ‘inaccessible patient’ ie altered GCS, obtunded or intellectually impaired/non communicative patients
- The affected compartment usually feels tense (unreliable in the obese an unreliable for ruling out compartment syndrome)
- Pain on passive extension of that compartment’s muscles
- Parasthesias (late)
- Pallor(late)
- Poikilothermia/Perishing cold (late)
- Pulselessness/Diminished pulses (late)
- Paralysis (late)
Investigations
- Diagnosis is clinical but can be confirmed by measuring intracompartmental pressures by either using a pressure monitor (call ortho reg and/or obtain from theatre) or arterial line pressure transducer (may need to be done in recovery)
- Check FBC, UEC, CK and urine myoglobin
Management
- Remove constricting dressings including tourniquets . Apply direct pressure if any bleeding
- Reduce fractures
- Treat pain
- Fasciotomy of the affected compartment is the definitive management and not regional anaesthesia/blockade
Degloving injuries
Degloving injuries occur when the skin and soft tissues is peeled away off the underlying fascia exposing the underlying structures (like taking off a glove). A common example is finger degloving caused by a ring which catches on a structure and pulls the skin away (eg: from swinging on a bar). It is also common in mangled lower legs.
The wounds should be irrigated and covered in saline soaked gauze.
Antibiotics should be administered and tetanus updated.
Gently irrigate any detached skin and wrap in saline soaked gauze
Replantation of the skin might be possible – early referral to plastic surgery is essential (after other life threats have been identified and managed). Some patients may require grafts, flaps or amputation.
It is possible to have a closed degloving injury where the overlying skin is still intact. They present with swelling, tenderness and fluctuance, but often little bruising. There is a risk of skin necrosis proportional to the size of the area affected and energy imparted. If no underlying fractures, it can be observed locally by the orthopaedic service and conservatively managed but can be discussed non-emergently as an acute referral with the on call Plastics referral.
Disposition – interhospital transfer guidelines
Definitive destination will depend on the site and type of injury. Critical ischaemia of a limb is the most emergent element of an injury and takes precedence.
Vascular injuries of the limbs
Upper Limb:
- Proximal forearm and above require Vascular Surgical intervention
- Forearm and distal to this require the Hands/Plastics service based at MMH.
Lower Limb:
- Proximal to the trifucation require Vascular Surgical intervention and may be considered for re-vascularisation depending on location of injury, age of the patient (and comorbidities) and associated injuries to both patient and limb. This is to be discussed with the On Call Vascular service.
- Critical ischaemia due to trauma below the trifurcation (lower leg) implies massive injury to the limb and will be treated with amputation in almost all adult cases. This may require discussion with the on-call Regional Plastic Service at MMH or on call Vascular service, but can be dealt with by the nearest Orthopaedic department.
Soft tissue defects in lower limb fractures
- If it is immediately apparent (at the roadside or in the emergency room of any upper North Island hospital other than MMH) that any open fracture will require Plastic Surgical intervention/limb salvage and other injuries do not take priority, it requires immediate referral and transfer to Middlemore Hospital.
- Whether to transfer is decided by the referring (not receiving) service. Early care (EMST/resuscitation, access, antibiotics, documentation, etc) and hand over to MMH (see below) must be complete.
- Open fractures requiring Plastic Surgical input are not always immediately apparent and may not be realised until after debridement at the local Orthopaedic centre. They then require urgent referral and transfer to the OrthoPlastic service at MMH via the on-call Orthopaedic AND Plastics service. It will be accepted by Orthopaedics.
- Referral and transfer requires informing both the On call Orthopaedic and Plastic Surgical registrars of the transfer. A referral through the on-line Plastics email account will also be required to transfer photographs of the injury. This must not delay transfer.
- Transfer must occur as early as possible, including on weekends, public holidays and out of hours to facilitate early intervention and optimal outcome.
- No CT is required prior to transfer. The first CT acquired should be after the first debridement, whilst in provisional fixation (usually external fixation) and should be a CTA of the injured limb.
- The patient will be admitted under the Orthopaedic on call team of the day and will be accepted by the Plastic Surgical team of the day. The transfer to the OrthoPlastic service will be internally managed on the next working day.
- The patient will be transferred as early as possible in the day, starved, to enable surgery at Middlemore on the same day. This facilitates timely management and better outcomes.
Contact numbers:
- Emergent Vascular Intervention: 0800 4 TRAUMA
- Orthopaedic reg at MMH: 021 594 764
- Plastic Surgical registrar at MMH on 021 784 057
References
- BOAST Standards
https://www.boa.ac.uk/standards-guidance/boasts/trauma-boasts.html - A Reevaluation of the Risk of Infection Based on Time to Debridement in Open Fractures J Bone Joint Surg Am 2021 Feb 3;103(3):265-273.
About this guideline
First published: February 2018 (Author: Emma Batistich)
Updated: May 2023 (EB), Oct 2023 (EB), May 2024 (Rob Orec)
Approved by: Northern Region Trauma Network,Health New Zealand | Te Whatu Ora – Northern Region, NRHL, St John
Review due: 2 years