Thoracostomy considerations
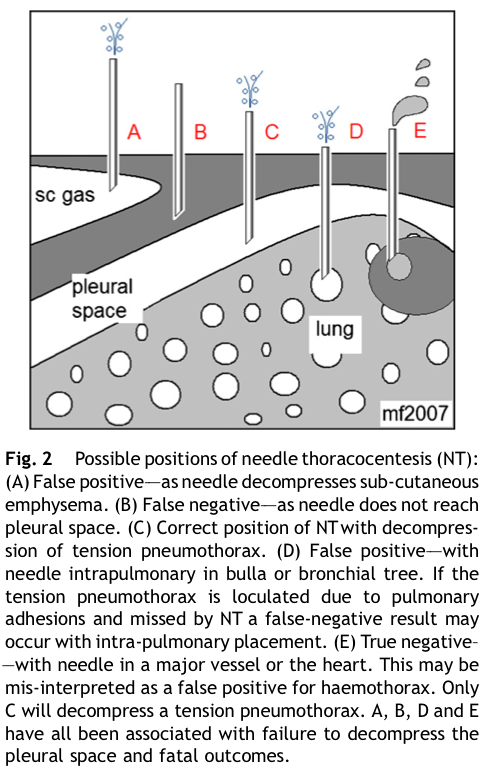
Needle thoracocentesis for tension pneumothorax
In a patient with a suspected tension pneumothorax, traditional trauma teaching advocated for rapid decompression on the affected side with a 14-16G needle in the 2nd intercostal space in the mid clavicular line.
The issues
There is a growing body of evidence that this may be ineffectual, is often misplaced, and can cause iatrogenic injury to the great vessels and lung.1,2
While needle thoracentesis can be considered as a temporising measure, especially in situation where performing a standard chest decompression is not possible, a rapidly performed thoracostomy using a scalpel in the 4th-5th intercostal space in the anterior axillary line should be performed preferentially in patients with a suspected tension pneumothorax or massive haemothorax.
If a needle thoracocentesis is performed, many now advocate placement in the 5th intercostal space in the anterior axillary line.
Empiric antibiotics for chest drain placement
Chest drain insertion after chest trauma is often associated with high rate of complications. The reported incidence of infectious complications following chest tube insertion for thoracic injuries ranges from 2 to 25 percent. Although the use of peri-operative prophylactic antibiotic therapy is well established, the use of prophylactic antibiotics for chest tube placement remains controversial.
Previous systematic reviews of prophylactic antibiotics in patients with penetrating and blunt chest injuries requiring the insertion of a chest drain concluded that they were associated with a reduced risk for post-traumatic empyema and pneumonia.
However a recent large prospective multi-centre trial of 1887 patients with traumatic hemopneumothorax has concluded that there is insufficient published evidence to support any recommendation either for or against the use of presumptive antibiotics to reduce the incidence of empyema or pneumonia in TT for traumatic hemopneumothorax.3
References
- Fitzgerald M, et al. Pleural decompression and drainage during trauma reception and resuscitation. 2008 Jan;39(1):9-20.
- Major trauma: assessment and initial management. NICE guideline. Published: 17 February 2017
- Cook A, Hu C, Ward J for the AAST Antibiotics in Tube Thoracostomy Study Group, et al Presumptive antibiotics in tube thoracostomy for traumatic hemopneumothorax: a prospective, Multicenter American Association for the Surgery of Trauma Study Trauma Surgery & Acute Care Open 2019
About this guideline
Published: February 2018
Author: Emma Batistich
Updated: Scott Cameron (April 2021)
Approved by: Northern Region Trauma Network, ADHB, WDHB, CMDHB, NDHB, NRHL, St. John
Review due: 2 years